Dr. Kelly Research Lab

Kelly GBM Lab which the Kvisle Fund has directed funds
ACF Report May 2021
Glioblastoma Organoids: A Novel 3-Dimensional model system for developing personalized therapy for Glioblastoma
Development and expansion of a GBM and Cancer organoid biobank
Our biobank of GBM organoids has continued to grow significantly over the past year. We continue to expand the biobank and have access to a diverse set of primary and recurrent GBM organoids. One of the key developments has been acquisition of a number of matched primary and recurrent GBM samples from patients before and after treatment. This key resource is critically important to understanding how GBM varies within the same patient over time. Another important development in the biobank has been the acquisition of samples from systemic cancers and development of organoids from breast and ovarian cancer. Now that we have effectively established both breast and ovarian cancer they can be utilized for further research, drug sensitivity and resistance testing.
Characterization of GBM organoids at an individual patient level
2021 has started with a significant amount of work that has led to completion of the first step of our GBM organoid genomic project that seeks to examine GBM and matched patient organoids at the single cell level. This collaborative effort between the Kelly Lab and the lab of Marco Marra at the UBC Genome Sciences Centre generated extensive single cell genomic sequencing data on 10 primary GBMs and two tumors at recurrence. This work demonstrates that significant heterogeneity exists in GBM and matched GBM organoids both within and between individual patients. Our manuscript titled ‘Single-cell landscapes of primary glioblastomas and matched organoids and cell lines reveal variable retention of inter- and intra-tumor heterogeneity’ has been submitted for publication and is currently under review at the premiere cancer journal Cancer Cell, and has been uploaded to the preprint server biorxiv (https://www.biorxiv.org/search/Leblanc%252Bgbm). This work has provided the foundation for ongoing collaboration and genomic interrogation of GBM and matched organoids, and has demonstrated that GBM organoids are the model system that best recapitulates a patient’s disease.
Patient specific organoid based therapeutic screening and clinical trial of personalized therapy for GBM
Through this work, our team continues to develop and improve our methods and capabilities for pre-clinical screening of novel therapeutics for patients with GBM. We have made important progress on this front as we progress towards initiation of a highly unique and novel phase I clinical trial: Biomarker and tumor cell culture-driven pilot trial for treatment of recurrent glioblastoma. This trial will generate patient derived GBM organoids in our lab, perform concurrent targeted sequencing of each patient’s tumour, identify alterations that might respond to targeted therapies and screen each patient’s organoids for response to these targeted therapies. Finally, we will administer the most effective agent based on the organoid response, thereby enabling patients in Alberta to receive truly personalized therapies they would not otherwise have been able to receive. This groundbreaking investigator initiated clinical trial has received both approval and funding from the TBCC. The trial protocol is being finalized at the TBCC now and will be submitted to Health Canada as soon as the TBCC signs off. We anticipate Health Canada Approval and trial initiation early in 2022.
The Team
In July of 2020, we brought a new post-doctoral fellow, Shaghayegh (Sherry) Aslan Pour Kal Bolandi, on to the team. Sherry has already begun to make important research contributions to the lab and has also received both University of Calgary and Charbonneau Cancer Institute Post-doctoral scholarships to pursue her work in our lab. This summer Lucy Yang will return to the lab as an undergraduate summer student. Lucy has received a PURE award to carry out her research project. Day to day lab operations are carried out by our two outstanding technicians Martha Hughes and Dorothea Livingstone.
Through the generous support of both the Kvisle family and the Alberta Cancer Foundation the past year has seen great progress in the Glioblastoma Organoids Project. We aim to generate knowledge that will inform therapeutic screening and identification for patients with GBM thereby leading to faster identification of potentially effective therapeutic agents. Ultimately, with this work we aim to prolong survival and improve quality of life for patients with GBM. We are very grateful and appreciative of your ongoing support and we could not carry out this important work without it. We look forward to further success in the upcoming year.

Paula de Robles, left, Gloria Roldan Urgoiti and Wee Yong at the Tom Baker
Researchers study Vitamin B3 as potential treatment for deadly brain tumour
UCalgary collaboration brings together basic scientists and cancer specialists
Author: Quentin Collier, Department of Clinical Neuroscience
A vitamin that is commonly used to fortify breakfast cereals is being studied by Cumming School (CSM) researchers for its potential to benefit people diagnosed with glioblastoma.
The study involving niacin — also known as Vitamin B3 — has the potential to boost the body’s immune system to fight the devastating brain tumour, but researchers must first complete a phase l-II clinical trial to determine the optimal dose and uncover any side effects.
“We want to know if it is safe, if it can be added to the standard treatment, and what dose should be used — that's phase l,” says neuro-oncologist Dr. Gloria Roldan Urgoiti, MD, a clinical associate professor at the CSM who is the principal investigator of this study. “You cannot assume that, because it is something that is available over the counter, you can just combine it with the standard treatment safely.”
Glioblastoma 'difficult to keep at bay'
After the safe dose in identified, and if the trial does not encounter unexpected toxicities, a total of 58 patients will be included in phase II to evaluate if it is effective to slow tumour growth.
The study, offered at the Tom Baker Cancer Centre in Calgary to adults up to age 75, addresses the most common malignant brain tumour in adults. Approximately 50 new glioblastoma cases are diagnosed each year in Calgary and 90 per cent are IDH-wildtype, which is the main molecular subtype and the focus of the study.
“The main problem with glioblastoma is that, although we have treatments to control it, we have difficulty keeping it at bay,” says Dr. Paula de Robles, MD, a clinical assistant professor at the CSM and a neuro- oncologist at the Foothills Medical Centre. “And in the majority of the patients, the tumour will come back eventually.”
After diagnosis, which typically follows the onset of neurological symptoms, standard of care treatment includes surgery followed by radiation therapy and oral chemotherapy. Even with aggressive treatment, in the majority of the cases the tumour returns within a year from diagnosis, says de Robles.
“That is why we are hoping we can make a difference with this clinical trial because we're giving niacin early, to try to help the standard of care.”
Tumours compromise immune system
Like many groundbreaking clinical trials, the niacin study has a long history that includes years of meticulous basic science research and investigators who chose to look at the problem from a new perspective.
Dr. V. Wee Yong, PhD, a professor and researcher at the CSM, says his group’s early paper on glioblastoma — published in the journal Nature Neuroscience in 2014 — recognized that the immune system is compromised by the tumours. Instead of suppressing the tumour growth, the immune system is subverted and used to the tumour's advantage.
“Glioblastoma stops the immune system that is trying to attack the tumour, and then it goes even further and exploits it for its own growth.”
It was also noted that a type of cell in the brain called microglia — the immune cells of the central nervous system — were not functioning properly.
Can vitamin B3 give immune system a boost?
Numerous drugs have been studied around the world to attack glioblastoma — all with little success. Instead, Yong decided to look for a stimulator of microglia in order to rejuvenate the compromised immune cells.
“We had already screened a library of 1,040 compounds and discovered some that suppress activity in microglia — which we then brought into our multiple sclerosis (MS) work — because that's what you want to do in MS.”
But for glioblastoma, he wanted the complete opposite — a drug that would give the immune system a boost and let it battle the tumour like it was meant to do.
“And that was niacin — Vitamin B3,” he says.


In tissue culture, glioblastoma patient-derived tumour stem cells grow robustly as clusters, with each cluster containing in excess of 100 cancer cells. When exposed to niacin-stimulated immune cells, the tumour cells are stopped in their tracks.
Images from the Yong lab
Next step: clinical trial
Over a span of five years, his team, led by research associate Dr. Susobhan Sarkar, PhD, showed that when compromised microglia are treated with niacin these microglia could stop the growth of the glioblastoma stem cells in culture. The team then moved the research to mice.
“Most impressively, when mice harboring intracranial glioblastoma were treated with niacin together with temozolomide (which is the standard chemotherapy for glioblastoma) they had a very prolonged survival.”
But before the bench research (published in Science Translational Medicine in 2020) can be translated to bedside care, a clinical trial is required to test if the vitamin is safe in patients with glioblastoma and to study how the body reacts to it.
“I first engaged Dr. Paula de Robles, who then introduced me to Dr. Gloria Roldan Urgoiti — and those are my two clinical collaborators,” recalls Yong.
The trio started enrolling their first study participants in April.
“Many clinical trials that have been done in patients with glioblastoma, but unfortunately most have failed to show increased survival,” says de Robles.
So we always get excited when there's a new thing. People living with this diagnosis are excited, too.

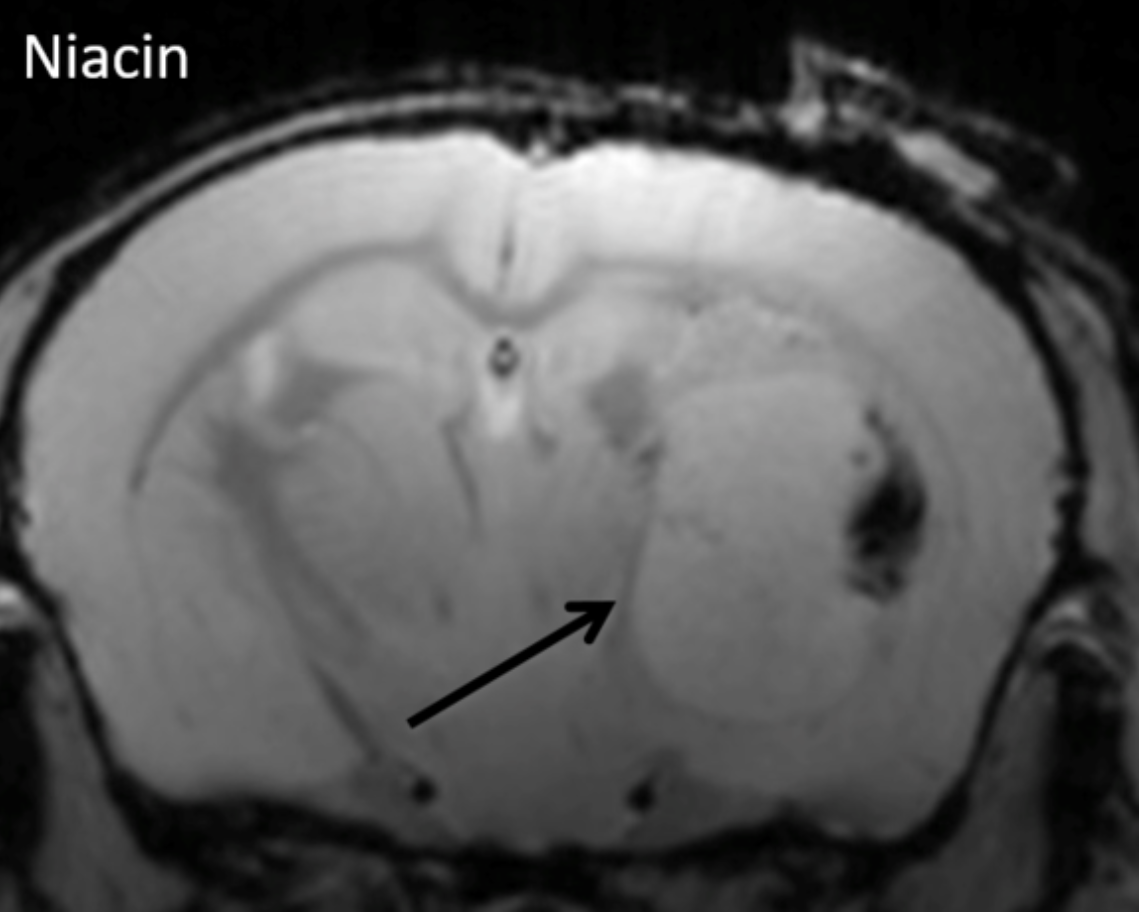
MRI shows that the huge growth capacity of glioblastoma tumour mass (arrow) within the brain in an experimental model was attenuated by niacin therapy compared to control.
Images from the Yong lab
Power of collaboration
In this phase l-II study, all participants will receive the drug concurrently to the standard of care. And though niacin has been used therapeutically in the past for the treatment of cholesterol, there are many unanswered questions that must be addressed before the research team can begin to measure the drug’s effect on the tumour.
“Can I tell you what will be the dose that they will tolerate? No,” says Roldan Urgoiti. “Can I tell you what is an effective dose? No — those are the answers that we hope the trial will give us.”
The entire project has been a testament to the power of collaboration between basic scientists and clinicians — and between members of different departments and institutes at the University of Calgary.
“Scientists alone can only take things so far,” says Yong. “We may have great ideas and great results published in top journals, but if you don't go on to show that it impacts humans, it is just another nice paper.”
Echoes Roldan Urgoiti: “This kind of research — which goes from the lab to the patient — is possible because we are in Calgary and we are in the University of Calgary. We have a very close relationship between the Charbonneau Institute, the Hotchkiss Brain Institute, and all the research areas.”
If the phase l trial is successful, phase ll will follow on to measure the effect of niacin on extending survival of patients with glioblastoma.
“There is always hope,” says Roldan Urgoiti. “We know it's a disease that we cannot cure, but we can always try to improve someone’s quality of life and help them live as long as possible.”
This Phase I/II study is supported by a foundation grant from the Canadian Institutes of Health Research, a gift from the Kvisle Fund through the Alberta Cancer Foundation, and developed with the support of the Clinical Research Unit at the Tom Baker Cancer Centre, Alberta Health Services.
Gloria Roldan Urgoiti is a clinical associate professor in the Department of Oncology at the CSM and a member of the Hotchkiss Brain Institute and the Arnie Charbonneau Cancer Institute.
Paula de Robles is a clinical assistant professor in the departments of Clinical Neurosciences and Oncology at the CSM and leader of the Tom Baker Cancer Centre Neuro-Oncology Program.
V. Wee Yong is a professor in the departments of Clinical Neurosciences and Oncology at the CSM and a member of the Hotchkiss Brain Institute and Arnie Charbonneau Cancer Institute.